

The System That Ate Healthcare
How aging populations, rising costs, and institutional inertia quietly reshaped medicine into one of the largest sectors of the modern economy.

📕Special note: The Billion Dollar Blindspot (the book) is almost ready to step into the world. If you want to follow the journey, early excerpts, behind-the-scenes notes, and launch news, you can sign up for early access here.
Here are 5 ways to support my work: 1. click “❤️” to amplify 2. subscribe 3. share this publication 4. buy me coffee 5. become a partner.
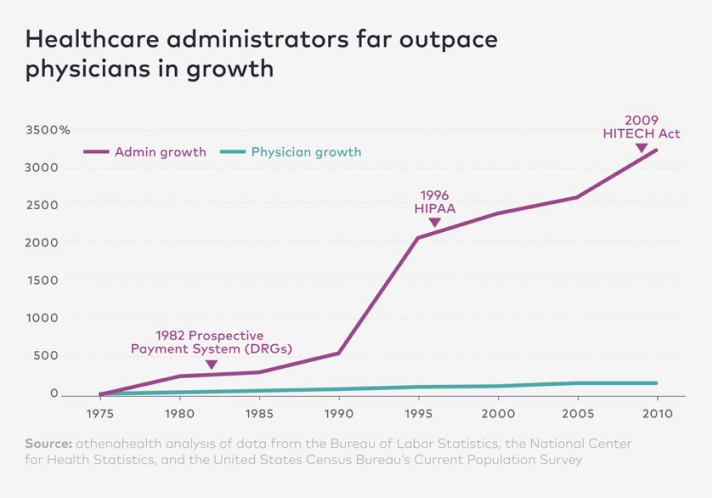
Between 1970 and 2010, employment in healthcare administration in the United States grew by roughly 3,200%. Over the same period, the number of physicians grew by only about 150%.
In essence, the workforce responsible for managing healthcare expanded more than twenty times faster than the workforce responsible for delivering it.
That mind-boggling statistic alone explains much of what many people instinctively feel when they interact with modern healthcare: the sense that the system is vast, complex, and strangely inefficient.

A physician friend once showed me what a routine appointment looks like from the other side of the exam room.
After a patient visit, he opened his electronic record system and started entering the information required to close the consultation: diagnosis codes, billing codes, insurance verification, compliance documentation, clinical summaries, and follow-up instructions.
Every step required another field, another form, another dropdown menu. By the time he finished entering everything, nearly ten minutes had passed. The appointment itself had lasted less than fifteen minutes.
“This,” he said quietly, gesturing toward the screen, “is where half my day goes.” Somewhere along the way, the infrastructure surrounding medicine had grown faster than medicine itself.
This system didn’t appear overnight. Its foundations were laid in the mid-1960s, when the United States introduced Medicare and Medicaid. The programs were designed to solve a pressing social problem: millions of Americans had little or no access to healthcare. To deliver care at scale, policymakers built a reimbursement infrastructure capable of financing medical services nationwide.
What followed over the next several decades was the gradual expansion of that infrastructure. Hospitals developed billing departments to navigate insurance claims. Insurers created detailed reimbursement frameworks requiring precise coding and documentation. Governments introduced compliance systems designed to prevent fraud and regulate quality. Health systems consolidated and expanded administrative oversight. Layer by layer, the system grew.
None of these changes was irrational in isolation; each one addressed a real problem. But together, they produced something few people originally intended: one of the most administratively complex systems in the global economy. Meanwhile, healthcare costs kept rising.
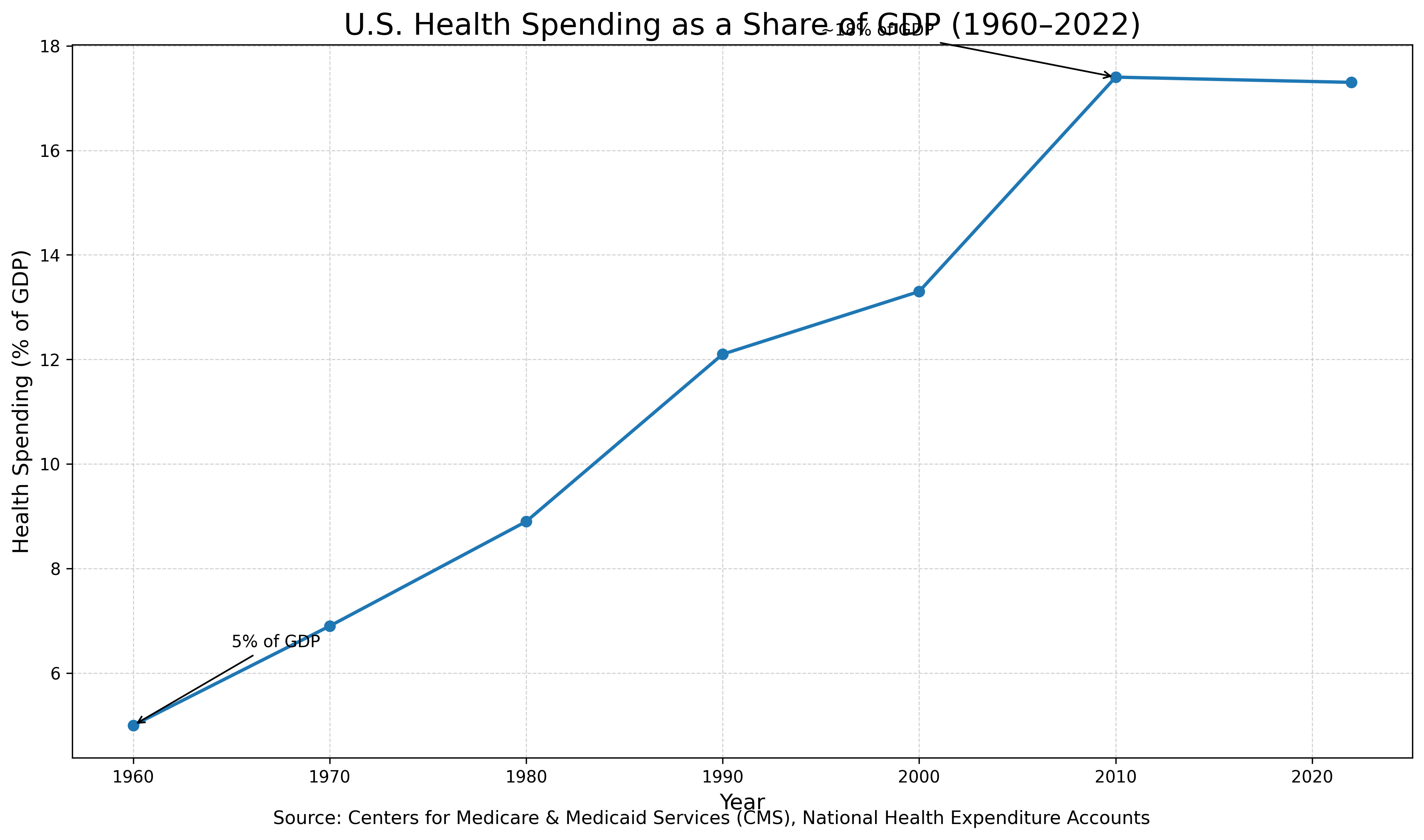
In 1960, healthcare spending in the United States accounted for about 5% of GDP. Today, it approaches 18%, making healthcare one of the largest sectors of the economy.
And yet despite that enormous scale, many healthcare systems still struggle to deliver efficient, accessible care. It’s a strange paradox. Healthcare has never been more technologically capable. Yet the system delivering it has never been more strained.
When industries accumulate complexity for long enough, something predictable tends to happen. Innovation begins to emerge at the edges. We’ve seen this pattern in many sectors. Financial systems built around traditional banks eventually gave rise to fintech platforms that offer faster, simpler services. The complexity of cable television paved the way for streaming platforms that fundamentally changed media distribution. Enterprise software systems weighed down by expensive infrastructure eventually gave way to cloud computing.
Healthcare has historically been slower to change than other industries for obvious reasons. Medicine is heavily regulated, and scientific breakthroughs take time. But friction eventually attracts innovation. And healthcare has accumulated decades of it.
Today, several powerful forces are converging inside the system.
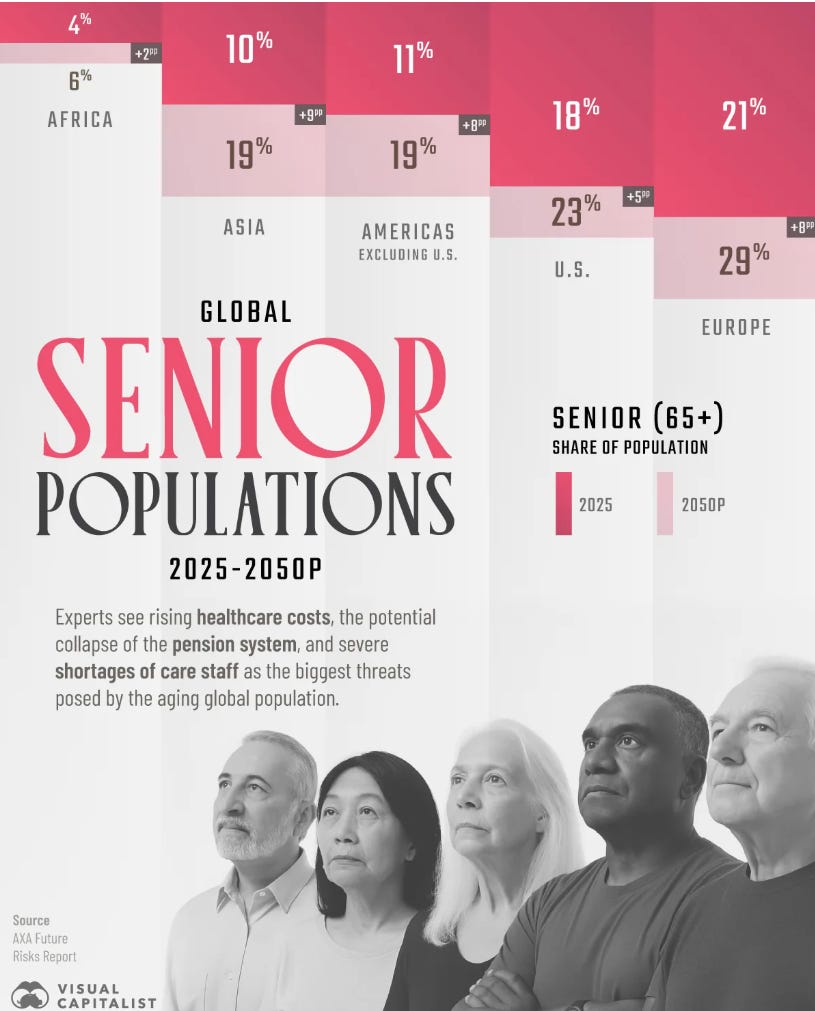
The first is demographic. Populations across developed economies are aging rapidly. In 1950, older adults represented a small minority of the global population. Today, they are approaching one in ten people worldwide. Within a generation, they will approach one in six. The structure of healthcare demand is changing faster than most health systems—or investment frameworks—have adjusted for.
The second is technological. Artificial intelligence, advanced diagnostics, wearable sensors, and data-driven medicine are beginning to reshape how healthcare can be delivered.
The third is cultural. Patients increasingly expect the same transparency, speed, and personalization from healthcare that they experience in other parts of the digital economy.
Taken together, these forces are beginning to reshape one of the world’s largest industries. But large transformations rarely unfold evenly. They tend first to expose the weaknesses of existing systems in specific places.
After two decades allocating capital across both public and private markets, one lesson has repeatedly held: identifying the broad trend is rarely the hardest part of investing. Markets are usually good at recognizing big themes. The more challenging question is where the opportunity actually lies.
Industries undergoing structural change rarely evolve uniformly. Instead, innovation tends to concentrate in the areas where the system has been slowest to adapt—places where demand has been underestimated, research has been limited, or capital has been historically scarce.
Healthcare contains several such areas. And some of them are much larger than most investors realize. Understanding those blind spots and the markets beginning to form around them is where the real investment story starts.
This essay is the first in a four-part series exploring the future of healthcare innovation and the investment opportunities emerging around it. In the next essays, I’ll examine:
Part II — The Blind Spot in Medicine
Why has one of the largest segments of healthcare demand historically received far less attention from research and capital than its economic significance would suggest?
Part III — Why Investors Miss the Biggest Opportunities
How structural incentives in venture capital and private markets often cause investors to overlook emerging sectors until they are already mature.
Part IV — The Real Art of Investing
Why identifying the opportunity is only the beginning, and why execution ultimately determines who captures it.
If you want the broader lens behind this framework, my upcoming book The Billion Dollar Blindspot explores how capital actually flows and why women’s health remains one of the most mispriced areas of healthcare investing.
Join Our Network
If you are building or backing credible, under-the-radar solutions in women’s health, we curate and occasionally review select opportunities with our investor community as part of our learning process. If your work would contribute meaningfully to that discussion, reach out privately.
I write weekly at The Billion Dollar Blindspot about capital, care, and the future of overlooked markets. If you are building, backing, or allocating in this space, I’d love to connect.
Disclaimer & Disclosure
This content is for informational and educational purposes only. It does not constitute financial, investment, legal, or medical advice, or an offer to buy or sell any securities. Opinions expressed are those of the author and may not reflect the views of affiliated organisations. Readers should seek professional advice tailored to their individual circumstances before making investment decisions. Investing involves risk, including potential loss of principal. Past performance does not guarantee future results.